Medicine Blended Assignment - May 2021
I have been given the following cases to solve
in an attmept to understand the topic of 'Patient clinical data analysis' to
develop my competency in reading and comprehending clinical data including
history, clinical findings, investigations and diagnosis and coem up with a
treatment plan.
This is the link of the questions asked
regarding the cases:
http://medicinedepartment.blogspot.com/2021/05/online-blended-bimonthly-assignment.html?m=1

1) Pulmonology (10 Marks)
A) Link to patient details:
https://soumyanadella128eloggm.blogspot.com/2021/05/a-55-year-old-female-with-shortness-of.html
Questions:
1) What is the evolution of the symptomatology in this patient in terms of an event timeline and where is the anatomical localization for the problem and what is the primary etiology of the patient's problem?
Ans- Evolution of symptomatology in this
patient is as follows-
- 20 years ago – 1st episode of shortness of breath
- Next 8 years – similar episodes 1/year ,lasting a week
- 12 years ago – a more severe episode of shortness of breath – hospitalized
- Next 12 years - similar episodes 1/year
- 8 years ago – diagnosed with diabetes
- 5 years ago – diagnosed with anemia
- 1 month ago – generalized weakness
- 20 days ago - diagnosed with hypertension
- 15 days ago - pedal edema and facial puffiness
Anatomical localization : LUNGS (bronchi and bronchioles) – lesions here led to increased pulmonary blood pressure thus causing Right Heart Failure.
Primary etiology :
• This condition is seen to reccur every year around the same time and area of work, thus suggesting that it is an allergic reaction to Paddy dust.
• Apart from that there is a history of use of CHULHA for years – which might have aggrevated the condition in following years.
Primary etiology of patient- Usage of chulha since 20 yrs might be
due to chronic usage .
2) What r the mechanism of action
indication(MOA) and efficacy over placebo of each of the phramacological and
nonphramacological interventions used for this patient?
Ans- Nonphramacological interventions-
1)
Head end elevation-
MOA- Improves oxygenation, decreases incidence VAP, increases hemodynamic
performance, increases end expiratory lung volume, decreases incidence of
aspiration.
Indication- Head injury, meningitis, pneumonia.
2)
O2 inhalation to maintain SPO2 above 92%-
3)
Intermittent BiPAP for 2hrs
MOA-
Assist ventilation by delivering positive expiratory and inspiratory
pressure with out need for ET incubation
Phramacological
interventions-
1)
Inj. AUGUMENTIN 1.2gm IV BO
MOA- THIS BLOCKS THE ACTION OF 𝜷
-LACTAMASE , POTASSIUM CLAVULANTA CAN BE INCORPORATED WITH AMOXICILLIN TO FORM
AUGUMENTIN.
INDICATIONS-
1)lower respiratory tract infection
2)acute bacterial otitis media
3)sinusitis
2)TAB. AZITHROMYCIN 500mg OD
MOA- Azithromycin binds to the 23S rRNA of the
bacterial 50S ribosomal subunit. It stops bacterial protein synthesis by
inhibiting the transpeptidation/translocation step of protein synthesis and by
inhibiting the assembly of the 50S ribosomal subunit
Indication- chest infections such
as pneumonia, infections of the nose and throat such as sinus infection
(sinusitis), skin infections, Lyme disease, and some sexually transmitted
infections.

3) What could be the causes for her current acute
exacerbation?
Ans- The most common cause of an exacerbation
is infection in the lungs or airways (breathing tubes). This infection is often
from a virus, but it may also be caused by bacteria or less common types of
organisms.
4) Could the ATT have affected her symptoms, if so
how?
Ans- Yes ATT affected her symptoms
Isoniazid and rifampcin can be nephrotoxic – Thus, raised
RFT was seen.
5) What could be the causes for her electrolyte
imbalance?
Ans-
RISK FACTORS
ACTIVATION OF RAS
[RENIN ANGIOTENSIN-ALDOSTERON SYSTEM]
ELEVATED PLASMA
ARGININE VASOPRESSIN
AGGREVATES
ELECTROLYTE IMBALANCE
Common causes- 1.RENAL INSUFFICIENCY
2.HYPOXIA
3.HYPERCAPNIA
4.RESPIRATORY
ACIDOSIS
5.RIGHT
SIDED HEART FAILURE
6.MALNOURISHED
2) Neurology (10 Marks) -
A) Link to patient details:
https://143vibhahegde.blogspot.com/2021/05/wernickes-encephalopathy.html
1) What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
Ans-
Evolution of the symptomatology in this patient in terms of an event timeline-
1-He had 2-3
episodes of seizures, one being 1 year ago and the most recent being 4 months
ago.
2-The most recent
time, (4 months ago), he had developed seizures (most probably GTCS) following
cessation of alcohol for 24 hours, which was associated with restlessness,
sweating, and tremors. Following this episode, he started drinking again.
3-He was unable
to lift himself off the bed and move around, and had to be assisted. It was
associated with a decrease in food intake since 9 days
4-He also had
short term memory loss since 9 days
The primary
etiology of the patient's problem- ALOCHOL
INTAKE
2) What
are mechanism of action, indication and efficacy over placebo of each of the
pharmacological and non pharmacological interventions used for this patient?
Ans- 1.
IVF NS and RL @150ml/hr
MOA- Sodium
Chloride is source of water and electrolytes. It is capable of inducing
diuresis depending on the clinical condition of the patient. It is a
crystalloid given intravenously in case of shock, dehydration, and diarrhoea to
increase the plasma volume.
Indication- The
following are primary indications for the use of normal saline infusion that
have been approved by the FDA: Extracellular fluid replacement (e.g.,
dehydration, hypovolemia, hemorrhage, sepsis) Treatment of metabolic alkalosis
in the presence of fluid loss. Mild sodium depletion
2. Inj. 1amp
THIAMINE in 100ml NS, TID
MOA- Thiamine
combines with adenosine triphosphate (ATP) in the liver, kidneys, and
leukocytes to produce thiamine diphosphate. Thiamine diphosphate acts as a
coenzyme in carbohydrate metabolism, in transketolation reactions, and in the
utilization of hexose in the hexose-monophosphate shunt.
Indications and
Usage-
Thiamine
hydrochloride injection should be used where rapid restoration of thiamine is
necessary, as in Wernicke's encephalopathy, infantile beriberi with acute
collapse, cardiovascular disease due to thiamine deficiency, or neuritis of
pregnancy if vomiting is severe.tion;
3. Inj. Lorazepam
MOA- Lorazepam
binds to benzodiazepine receptors on the postsynaptic GABA-A ligand-gated
chloride channel neuron at several sites within the central nervous system
(CNS). It enhances the inhibitory effects of GABA, which increases the
conductance of chloride ions into the cell
Indication- ATIVAN
Injection is indicated in adult patients for preanesthetic medication,
producing sedation (sleepiness or drowsiness), relief of anxiety, and a
decreased ability to recall events related to the day of surgery.
4. T. Pregabalin
75mg/PO/ BD
MOA- Pregabalin
has demonstrated anticonvulsant, analgesic, and anxiolytic properties in
preclinical models. The drug's exact mechanism of action is unclear, but it may
reduce excitatory neurotransmitter release by binding to the α2-δ protein
subunit of voltage-gated calcium channels
Indication- Pregabalin
is indicated for the management of neuropathic pain associated with diabetic
peripheral neuropathy, postherpetic neuralgia, fibromyalgia, neuropathic pain
associated with spinal cord injury, and as adjunctive therapy for the treatment
of partial-onset seizures in patients 1 month of age and older
5. Inj. HAI S.C.-
premeal
6. GRBS 6th
hourly, premeal: 8am, 2pm, 8pm,2am
7. Lactulose
30ml/PO/BD
MOA- Lactulose is
used in preventing and treating clinical portal-systemic encephalopathy. Its
chief mechanism of action is by decreasing the intestinal production and
absorption of ammonia. It has also gained popularity as a potential therapeutic
agent for the management of subacute clinical encephalopathy
Indication- Lactulose
is a prescription drug used by mouth or rectally to treat or prevent
complications of liver disease (hepatic encephalopathy). It does not cure the
problem, but may help to improve mental status. Lactulose is a colonic
acidifier that works by decreasing the amount of ammonia in the blood.
8. Inj 2 ampoule
KCl (40mEq) in 10 NS over 4 hours
MOA- Potassium
ions participate in a number of essential physiological processes, including
the maintenance of intracellular tonicity; the transmission of nerve impulses;
the contraction of cardiac, skeletal, and smooth muscle; and the maintenance of
normal renal function.
Indication- Potassium
chloride is used to prevent or to treat low blood levels of potassium
(hypokalemia). Potassium levels can be low as a result of a disease or from
taking certain medicines, or after a prolonged illness with diarrhea or vomiting.
3) Why
have neurological symptoms appeared this time, that were absent during
withdrawal earlier? What could be a possible cause for this?
Ans- Altered
sensorium due to alcohol withdrawal syndrome,
Decreased levels
of Thiamine lead to the symptoms.
4) What
is the reason for giving thiamine in this patient?
Ans- Thiamine
is a key vitamin in the maintenance of membrane integrity and osmotic gradients
across cell membranes and is stored in body tissues predominantly as thiamine
diphosphate (TDP). TDP participates in energy production as an essential
cofactor for several enzymes in the TCA cycle and pentose phosphate pathways
Thiamine
deficiency causes depletion of intracellular TDP, leading to a decreased
activity of the TCA cycle and pentose phosphate pathways. Consequently,
cellular energy (ATP) depletion and reduction of DNA/RNA and NADPH synthesis
ensues, which results in low resistance to oxidative stress. Moreover, there is
an accumulation of toxic intermediate metabolic products such as lactate,
alanine and glutamate, reduced cellular pH in cells, and disruption of the
homeostasis of cellular electrolytes, which results in cytotoxic edema.
5) What is the probable reason for
kidney injury in this patient?
Ans- Elevated levels of urea and creatinine are suggestive of Prerenal Azotemia being the most likely cause of kidney injury in this patient. This can be a result of decreased blood flow to the kidneys possibly due to dehydration secondary to Alcoholism.
6) What is the probable cause for
the normocytic anemia?
Ans- The possible causes of anemia can be the following:
- · Chronic
alcohol dependence causing decreased erythropoiesis as there is a direct toxic
effect of alcohol on the bone marrow
- · Anemia
can be secondary to poor nutrition and malabsorption syndrome
- · Alcoholic
gastritis that could have caused a hemorrhage in the stomach leading to loss of
blood
- · Possibility
of liver cirrhosis that could have caused sequestration of RBCs in spleen
7) Could chronic alcoholism have
aggravated the foot ulcer formation? If yes, how and why?
B) Link to patient details:
https://kausalyavarma.blogspot.com/2021/05/a-52-year-old-male-with-cerebellar.html?m=1
Questions-
1) What is the
evolution of the symptomatology in this patient in terms of an event timeline
and where is the anatomical localization for the problem and what is the
primary etiology of the patient's problem?
Ans- The
evolution of the symptomatology in this patient in terms of an event timeline
1.History of
giddiness associated with 1 episode of vomiting on the same day.
2.This was
associated with Bilateral Hearing loss, aural fullness and presence of
tinnitus.
3.He has
associated vomiting- 2-3 episodes per day, non projectile, non bilious
containing food particles.
4.Patient has H/o
postural instability- he is unable to walk without presence of supports,
swaying is present and he has tendency to fall while walking.
Primary
Etiology-
Obstruction of
the posterior inferior cerebellar artery (PICA, also the most frequent location
for a cerebellar infarct) leads to a headache and less commonly vomiting,
vertigo, horizontal ipsilateral nystagmus, and truncal ataxia.
Anterior inferior
cerebellar artery (AICA) territory infarction more often leads to dysmetria,
Horner's syndrome, unilateral hearing loss and ipsilateral facial paralysis or
anesthesia with contralateral hemibody sensory loss of pain and temperature.
Finally,
obstruction of the superior cerebellar artery (SCA, located most rostral) tends
to produce more ataxia, dysarthria, and nystagmus, with less vertigo, headache,
and vomiting.
However,
presentations can often be atypical or overlap, in particular for hemorrhagic
infarcts.
2) What
are mechanism of action, indication and efficacy over placebo of each of the
pharmacological and non pharmacological interventions used for this patient?
Ans- Pharmacological interventions-
1. Tab Veratin 8
mg PO TID
MOA- Betahistine
is one of the few drugs known which is said to improve the microcirculation of
the inner ear. It works as a histamine analogue through 2 modes of action(1)
agonist of H1 receptors and (2) antagonist of H3 receptors. It has a weak
effect on H1 receptors but strong effect on H3 receptors.
Indication- Vertin
Tablet is used to prevent and treat a disorder of the inner ear known as
Ménière's disease. The symptoms include dizziness (vertigo), ringing in the
ears (tinnitus), and loss of hearing, probably caused by fluid in the ear.
2. Inj Zofer 4 mg
IV/TID
MOA- Zofer
Injection works by inhibiting the action of a chemical substance known as
serotonin. Serotonin is responsible for inducing nausea and vomiting.
Ondansetron binds to a receptor known as 5-HT₃, thus inhibits the binding of
serotonin to it and prevents vomiting and nausea.
3. Tab Ecosprin
75 mg PO/OD
MOA- Ecosprin is
an antiplatelet medicine. It works by inhibiting the action of an enzyme, which
makes platelets aggregate together to form a blood clot.
Indication- This
tablet is also used to prevent heart attacks, stroke and heart-related chest
pain (angina)
4.Tab
Atorvostatin 40 mg PO/HS
MOA- Atorvastatin
competitively inhibits 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA)
reductase. By preventing the conversion of HMG-CoA to mevalonate, statin
medications decrease cholesterol production in the liver
Indication- Reduce
the risk of non-fatal myocardial infarction.
Reduce the risk
of fatal and non-fatal stroke.
Reduce the risk
for revascularization procedures.
Reduce the risk
of hospitalization for CHF.
Reduce the risk of angina.
5. Tab
Clopidogrel 75 mg PO/OD
MOA- The active
metabolite of clopidogrel selectively inhibits the binding of adenosine
diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP-
mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting
platelet aggregation. This action is irreversible.
Indication-FDA-approved
indications for clopidogrel include: Use during a percutaneous coronary
intervention (PCI) for acute coronary syndrome (ACS) and stable ischemic heart
disease. Primary prevention of
thromboembolism atrial fibrillation
Non-Pharmacological
interventions-
1. BP
monitoring- 4rth hourly
3) Did
the patients history of denovo HTN contribute to his current condition?
Ans-
Yes
4) Does
the patients history of alcoholism make him more susceptible to ischaemic or
haemorrhagic type of stroke?
Ans-
Yes, the patient has H/O chronic alcoholism and is susceptible to ischaemic
type of stroke.
C) Link to patient details:
http://bejugamomnivasguptha.blogspot.com/2021/05/a-45-years-old-female-patient-with.html
Questions:
1) What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
Ans-
Evolution of symptoms-
1.Patient was
normal 8 months back then developed b/l pedal edema which gradually progressed.
(Aggerevated in sitting and standing position, relived on taking medication)
2.Palpitations : since
5days, sudden in onset which is more during night
(Aggerevated by
lifting heavy weights, speaking continuously)
3.Dyspnoea during
palpitations (NYHA-3) since 5 days
4.Pain: since
6days, radiating along left upper limb, more during palpitations and relived on
medication.
5.Chest pain
associated with chest heaviness since 5 days
Etiological agent
-Electrolyte imbalance (hypokalemia) causing the her manifestations like palpitations, chest
heaviness, generalised body weakness.
Radiating pain
along her left upper limb due to cervical spondylosis.
2) What are the reasons for
recurrence of hypokalemia in her? Important risk factors for her hypokalemia?
Ans-
Reason: recurrent hypokalemic periodic paralysis
Current risk
factor:due to use of diuretics
Other risk
factors
A) Medications-diuretics,
laxatives, enema, corticosteroids causes- osmotic diuresis, mineralo corticoid
excess, renal tubular acidosis, hypomagnesenemia
B) Trans-cellular
shift : alkalosis, thyrotoxicosis, delirium tremans, head injury, Myocardial,
ischemia, recurrent hypokalemic periodic paralysis
C) Inadequate
intake: anorexia, dementia, stareation, total parental nutrition
D) Psuedohypokalemia:
delayed sample analysis, significant leukocytosis.
3) What are the changes seen
in ECG in case of hypokalemia and associated symptoms?
Ans- Changes seen in ECG-
Earliest change- Decreased T-wave amplitude, ST depression,
Twave - and inversion or flat;prolonged PR interval;presence of Uwaves
In Severe cases- ventricular fibrillation, rarely AV block
Symptoms of hypokalemia-
Weakness & fatigue, palpitations, muscle cramps &
pain, anxiety, psychosis, depression, delirium.
D) Link to patient details:
https://rishikoundinya.blogspot.com/2021/05/55years-old-patient-with-seizures.html
QUESTIONS:
1) Is there any
relationship between occurrence of seizure to brain stroke. If yes what is the
mechanism behind it?
Ans-
Yes. Seizures after haemorrhagic strokes are thought to be attributable to
irritation due to Hemosiderin deposits caused by products of blood metabolism.
2) In the previous episodes of
seizures, patient didn't loose his consciousness but in the recent episode he
lost his consciousness what might be the reason?
Ans- Initially the patient might have
had Simple partial seizures (no loss of consciousness) and might have
progressed to Generalised Tonic Clonic seizures (loss of consciousness).
E) Link to patient details:
https://nikhilasampathkumar.blogspot.com/2021/05/a-48-year-old-male-with-seizures-and.html?m=1
Questions:
1) What could have been the reason for this patient to develop ataxia in the past 1 year?
Ans- The patient has minor unattended head injuries in the past 1 yr. Accoding to the CT scan, the patient has cerebral haemorrhage in the frontal lobe causing probably for the occurrence of Frontal love ataxia.
2) What was the reason for his IC bleed? Does Alcoholism contribute to bleeding diatheses ?
Ans- The patient has minor unattended
head injuries. During the course of time the minor hemorrhages if present
should have been cured on their own. But the patient is a chronic alcholic.
This might have hindered the process of healing or might have stopped the
healing rendering it to grow further more into 13 mm sized hemorrhages
occupying Frontal Parietal and Temporal lobes.
F) Link to patient details:
Questions:
1) Does the patient's
history of road traffic accident have any role in his present condition?
Ans- The closeness of facial bones to the cranium would suggest that there are chances of cranial injuries. Since the Zygomatic arch and Mandibular process is very close to the cranium, this might play a role in the patient's present condition.
2) What are warning
signs of CVA?
Ans- Weakness or numbness of the face, arm or leg,
usually on one side of the body
Trouble speaking or understanding
Problems with vision, such as dimness or loss of vision in one or both
eyes
Dizziness or problems with balance or coordination
Problems with movement or walking
Fainting or seizure
Severe headaches with no known cause, especially if they happen suddenly
3) What is the drug
rationale in CVA?
Ans- 1.Mannitol-
Because of its osmotic effect, mannitol is assumed to decrease cerebral edema. Mannitol might improve cerebral perfusion by decreasing viscosity, and as a free-radical scavenger, it might act as a neuroprotectant.
2.Ecospirin-
For the prevention of heart attack, stroke, heart conditions such as stable or unstable angina (chest pain) due to a blood clot.
3.Atrovastin- Atorva 40 Tablet belongs to a group of medicines called statins. It is used to lower cholesterol and to reduce the risk of heart diseases. Cholesterol is a fatty substance that builds up in your blood vessels and causes narrowing, which may lead to a heart attack or stroke.
4.RT feed- RT feed is a nursing procedure to provide nutrition to those people who are either unable to obtain nutrition by mouth or are not in a state to swallow the food safely.
4) Does alcohol has
any role in his attack?
Ans- When the patient met with an accident there might
be cranial damage which was unnoticed.
If so his occasional drinking may or may not have hindered the process
of the minor hemorrhages getting healed and might have caused this condition
But since the patient is not a chronic alcoholic and so Alcohol might
not have played any role.
Therefore it cannot be evaluated without further details.
5) Does his lipid
profile has any role for his attack?
Ans- The inverse relationship between serum HDL-C and
stroke risk . When taken together it seems clear that higher baseline levels of
serum HDL-C lower the risk of subsequent ischemic stroke.
G) Link to patient details:
https://amishajaiswal03eloggm.blogspot.com/2021/05/a-50-year-old-patient-with-cervical.html
QUESTIONS:
1)What is myelopathy hand ?
Ans- There is loss of power of
adduction and extension of the ulnar two or three fingers and an inability to
grip and release rapidly with these fingers. These changes have been termed
"myelopathy hand" and appear to be due to pyramidal tract
involvement.
2)What is finger
escape ?
Ans- Finger escape
sign or Wartenberg's sign is a neurological sign consisting of involuntary
abduction of the fifth (little) finger, caused by unopposed action of the
extensor digiti minimi.
This finding of
weak finger adduction in cervical myelopathy is also called the "finger
escape sign"
3)What is Hoffman’s
reflex?
Ans- Hoffman's sign or reflex is a
test used to examine the reflexes of the upper extremities. This test is a
quick, equipment-free way to test for the possible existence of spinal cord
compression from a lesion on the spinal cord or another underlying nerve
condition.
H) Link to patient details:
https://neerajareddysingur.blogspot.com/2021/05/general-medicine-case-discussion.html?m=1
Questions-
1) What can be
the cause of her condition ?
Ans- Seeing that the patient is a young female, the
possible causes could include the following:
·
Trauma
·
Estroprogestative therapy ( oral
contraceptives)
·
Iron deficiency anemia
·
2) What are the risk
factors for cortical vein thrombosis?
Ans- The risk factors include the following:
·
Congenial or acquired heart diseases
·
Underlying Infection
·
Birth control pills use
·
Dehydration
·
Cancer
3)There was seizure
free period in between but again sudden episode of GTCS why?resolved
spontaneously why?
Ans- Underlying unresolved edema is the
probable cause for the recurrent precipitation of seizures. So when the edema
resolved, the seizure resolved spontaneously.
4) What drug was used
in suspicion of cortical venous sinus thrombosis?
Ans- Injection Clexane
was used to resolve the thrombosis and Mannitol infusion was given to bring down
cerebral edema.
3) Cardiology (10 Marks)
A) Link to patient details:
https://muskaangoyal.blogspot.com/2021/05/a-78year-old-male-with-shortness-of.html.
1)What is the difference btw
heart failure with preserved ejection fraction and with reduced ejection
fraction?
Ans- Preserved
ejection fraction (HFpEF) – also referred to as diastolic heart failure. The
heart muscle contracts normally but the ventricles do not relax as they should
during ventricular filling (or when the ventricles relax).
Reduced ejection
fraction (HFrEF) – also referred to as systolic heart failure
HFpEF is preceded
by chronic comorbidities, such as hypertension, type 2 diabetes mellitus
(T2DM), obesity, and renal insufficiency, whereas HFrEF is often preceded by
the acute or chronic loss of cardiomyocytes due to ischemia, a genetic
mutation, myocarditis, or valvular disease.
2)Why haven't we done
pericardiocenetis in this pateint?
Ans- Pericardiocentesis
is not done here Because the effusion was self healing ,It reduced from
2.4cm to 1.9 cm.
3)What are the risk factors for
development of heart failure in the patient?
Ans- Risk factors here
are-
1.Alcohol abuse
increases the risk of atrial fibrillation, heart attack and congestive heart
failure
2.High blood
pressure
3.Smoking
4.Diabetes
5.AV block can be
associated with severe bradycardia and hemodynamic instability. It has a
greater risk of progressing to third-degree (complete) heart block or asystole.
4)What could be the cause for
hypotension in this patient?
Ans- Visceral
pericardium may have thickened which is restricting the heart to expand
causing hypotension (May be secondary to TB).
B) Link to patient details:
https://muskaangoyal.blogspot.com/2021/05/a-73-year-old-male-patient-with-pedal.html.
Questions:
1.What are the
possible causes for heart failure in this patient?
Ans- The patient has
various comorbidities which could have led to a heart failure
- 1. The patient was diagnosed with type 2 diabetes mellitus 30 years ago and has been taking human mixtrad insulin daily and was also diagnosed with diabetic triopathy indicating uncontrolled diabetes which is major risk factor for heart failure
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5494155/
- 2.
The patient was also diagnosed with hypertension 19 yrs. ago which is
also a risk factor for heart failure
- https://pubmed.ncbi.nlm.nih.gov/31472888/
- 3.
He is a chronic alcoholic since 40 years which is a risk factor towards
heart failure
- https://www.nmcd-journal.com/article/S0939-4753(19)30360-6/fulltext
- 4.
The findings in this article provide longitudinal evidence that moderate
and heavy alcohol consumption are associated with decreased LVEF and trend
towards a higher risk of incident LV systolic dysfunction, compared to light
drinkers.
- The patient has elevated creatinine and AST/ALT ratios is >2 and was diagnosed with chronic kidney disease stage IV. CKD is also one of the risk factors for heart failure
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2900793/
2.what is the
reason for anaemia in this case?
Ans- Alcoholics
frequently have defective red blood cells that are destroyed prematurely,
possibly resulting in anemia. Alcohol also interferes with the production and
function of white blood cells, especially those that defend the body against
invading bacteria. Consequently, alcoholics frequently suffer from bacterial
infections which may lead to anemia.
3.What is the
reason for blebs and non healing ulcer in the legs of this patient?
Ans- The patient had recurrent blebs and ulcer on lower limbs (foot). This is due to Type-2 diabetes mellitus.
Diabetic foot ulcers generally arise as a result of poor circulation in the foot region. While high blood sugar levels and nerve damage or even wounds in the feet may result in foot ulcers in many cases.
In cases of poor circulation of blood, the foot ulcers take quite a bit of time to heal as the blood efficiency in the foot region is at a low level. Furthermore, many develop a bit of reduced sensation on the feet as a result of nerve damage or more.
There are many risk
factors that may lead to foot ulcers at the end-
- 1. Poor quality or fitting of the footwear.
- 2. Unhygienic
appearance of foot.
- 3. Improper care of
the nails of the toe.
- 4. Heavy intake of
alcohols and tobacco.
- 5. Obesity and
Weight-related
- 6. Complication
arising from Diabetes like eye problems, kidney problems and more.
- 7.
Although aging or old age can also be counted among them.
4. What sequence of
stages of diabetes has been noted in this patient?
Ans- Sequence of
stages here is-
- 1.
Alcohol abuse
- 2. Obesity
- 3. impaired glucose
tolerance
- 4. diabetes mellitus
- 5. microvascular
complications like triopathy and diabetic foot ulcer
- 6.
macrovascular complications like coronary artery disease , coronary
vascular disease and peripheral vascular disease.
C) Link to patient details:
https://preityarlagadda.blogspot.com/2021/05/biatrial-thrombus-in-52yr-old-male.html
1) What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
Ans- Evolution of symptomatology-
- 1. Facial puffiness ( since 2 to 3 yrs)
- 2. SOB grade 2( 1yr ago)
- 3. SOB grade 2( 2days back again)
- 4. SOB grade 4
- 5. Decreased urine output ( since 2
days)
- 6. Anuria (since morning)
Anatomical localisation:- Atrial Septum
Primary etiology:-
- 1. Atrial Septal defect leading to Atrial Fibrillation
- 2. Atrial fibrillation caused stagnation of blood and hence thrombus formation
- 3. Atrial septal defect also caused shunting from left to right atrium causing pulmonary hypertension
- 4. Pulmonary Hypertension caused reversal of shunting and hence increased stagnated pool of blood contributing to thrombus formation and Congestive Cardiac failure.
2) What are mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non
pharmacological interventions used for this patient?
Ans- 1.Dobutamine-
MOA: acts on beta 1 receptor
Beta1 ionotropic effect →
increases heart contractility → increases cardiac output
Indications- Cardiogenic shock ,
Reversible heart failure
2.Digoxin-
MOA: Digoxin has two principal
mechanisms of action which are selectively employed depending on the
indication: Positive Ionotropic: It increases the force of contraction of the
heart by reversibly inhibiting the activity of the myocardial Na-K ATPase pump,
an enzyme that controls the movement of ions into the heart.
Indications- Atrial fibrillation ,atrial flutter, Heart
failure,Abortion
3.Heparin- MOA: Produces an anticoagulant
effect by inhibiting activated factor X and thrombin and hence prevents fibrin
formation
Indication: The patient had thrombi in
left atrium and left appendages
3) What is the pathogenesis of
renal involvement due to heart failure (cardio renal syndrome)? Which type of
cardio renal syndrome is this patient?
Ans- Pathogenesis of cardiorenal
syndrome is described below in the picture:
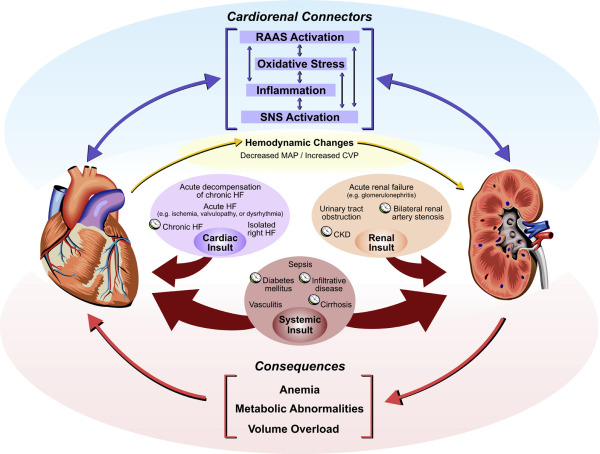
Stage 3 cardio renal
syndrome is seen in this patient.
4) What are the risk factors for
atherosclerosis in this patient?
Ans- Hypertension is the risk factor
for atherosclerosis in this patient.
5) Why was the patient asked to
get those APTT, INR tests for review?
Ans- The patient was asked to get
those APTT, INR tests for review because of Thrombosis and to check on
development of thrombosis.
D) Link to patient details:
Questions-
1) What is the
evolution of the symptomatology in this patient in terms of an event timeline
and where is the anatomical localization for the problem and what is the
primary etiology of the patient's problem?
Ans- Event timeline:
- 1. Heartburn
since 1 year
- 2. Tuberculosis
7 months ago
- 3. Shortness
of breath since 30 minutes
Anatomical localisation:
Coronary vessels
Primary etiology:
- 1. Type
2 diabetes mellitus
- 2. Hypertension
2) What are mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non
pharmacological interventions used for this patient?
Ans- The treatment modality used in this patient is-
Metoprolol:-
MOA: Acts of beta receptor, creates negative
chronotropic and ionotropic effect
Indication: Patient is hypertensive with LV
dysfunction.
3) What are the indications and
contraindications for PCI?
Ans- Indications- .
- 1.ST-elevation myocardial infraction(STEMI)
- 2.Atypical chest pain,
- 3.Stable angina,
- 4.Unstable angina,
- 5.Positive stress test
- 6.Non ST-elevation myocardial infarction
Contraindications-
- 1.Lack of cardiac support
- 2.Coagulopathy
- 3.Hypercoagulable states
- 4.Critical left main coronary stenosis without collateral flow from a native vessel or previous bypass graft to the left anterior descending artery
- 5.Diffusely diseased vessel without focal stenosis
- 6.A single diseased vessel providing all perfusion to the myocardium
- 7.Total occlusion of a coronary artery
- 8.Stenosis <50%
4) What happens if a PCI is
performed in a patient who does not need it? What are the harms of
overtreatment and why is research on overtesting and overtreatment important to
current healthcare systems?
Ans- The 2013 American
College of Cardiology Foundation/American Heart Association (ACCF/AHA)
guidelines for the management of STEMI consider primary PCI as a class I
indication in STEMI patients within 12 hours’ of initial symptom onset.2 Beyond
this timeframe PCI does not show benefit, as shown in the occluded artery trial
which evaluated PCI benefit among stable, high-risk patients with persistent
total coronary occlusion after MI.
E) Link to patient details:
https://bhavaniv.blogspot.com/2021/05/case-discussion-on-myocardial-infarction.html?m=1
Questions:
1) What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
Ans- Evolution of symptomatology:
1. Uncontrolled DM2 since 8 years
2. 3 days back Mild chest pain
dragging type and retrosternal pain(radiated)
Anatomical localisation:- Inferior wall of heart
Primary etiology:- Diabetes type 2 (uncontrolled)
High blood glucose from diabetes
can damage your blood vessels and the nerves that control your heart and blood
vessels.
2) What are mechanism of action,
indication and efficacy over placebo of each of the pharmacological and non
pharmacological interventions used for this patient?
Ans- 1.TAB. ASPIRIN 325 mg PO/STAT
Mechanism of action: The acetyl group of
acetylsalicylic acid binds with a serine residue of the cyclooxygenase-1
(COX-1) enzyme, leading to irreversible inhibition. This prevents the production
of pain-causing prostaglandins.
2.TAB ATORVAS 80mg PO/STAT
Mechanism of action: Atorvastatin
competitively inhibits 3-hydroxy-3-methylglutaryl-coenzyme A (HMG-CoA)
reductase. By preventing the conversion of HMG-CoA to mevalonate, statin
medications decrease cholesterol production in the liver.
3.TAB CLOPIBB 300mg PO/STAT
Mechanism of action: The active
metabolite of clopidogrelselectively inhibits the binding of adenosine
diphosphate (ADP) to its platelet P2Y12 receptor and the subsequent ADP-
mediated activation of the glycoprotein GPIIb/IIIa complex, thereby inhibiting
platelet aggregation. This action is irreversible.
4.VITAL MONITORING.
3) Did the secondary PTCA do any
good to the patient or was it unnecessary?
Ans- Secondary PTCA provides a
valuable, safe and cost-effective way of management for recurrence of stenosis
after initially successful angioplasty. It increased the percent of patients
with documented long-term success of angioplasty
Over testing and over treatment
can raise a person’s risk of cardiovascular death by as much as four times.
F) Link to patient details:
https://kattekolasathwik.blogspot.com/2021/05/a-case-of-cardiogenic-shock.h
1. How did the
patient get relieved from his shortness of breath after i.v fluids
administration by rural medical practitioner?
Ans- Patient got relieved from his SOB due to
administration of IV fluids.
Because of the fluid loss
occurred to the patient there is decreased preload- so, SOB occurred due to
decreased CO
IV fluids administered- there is increased preload- SOB decreased due to
better of cardiac output.
2. What is the
rationale of using torsemide in this patient?
Ans- Torsemide is a
high efficacy diuretic which works by blocking Na-K-2Cl cotransporter, causing
their excretion and hence creating diuresis.
It was used in the patient as he was suffering from
pulmonary edema and it caused diuresis helping reduce the fluid volume
3. Was the rationale for administration of
ceftriaxone? Was it prophylactic or for the treatment of UTI?
Ans-As there was
presence of pus cells in urine, there was a suspicion of UTI. In order to
prevent its aggrevation, Ceftriaxine was given for its treatment.
4) Gastroenterology (& Pulmonology) 10 Marks
A) Link to patient details:
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-pancreatitis-with.html
QUESTIONS:
1) What is the evolution of the
symptomatology in this patient in terms of an event timeline and where is the
anatomical localization for the problem and what is the primary etiology of the
patient's problem?
Ans- Given
below is the timeline of symptom occurrences in the patient:-
1. Incident
of abdominal pain and vomiting 5 years ago following which there was cessation
of alcohol
2. 3
years ago resumed alcohol consumption and had another episode of pain abdomen
and vomiting
3. 5-6
episodes of abdominal pain in the past 1 year
4. 20
days ago started binge drinking
5. Abdominal
pain and vomiting since 1 week
6. Fever
and burning micturition since 4 days
Anatomical localization:
1. Sub-hepatic
region
2. Body
of the pancreas
3. Left
basilar segment of lung
Primary etiology:
Chronic alcohol consumption
2) What is the efficacy of drugs
used along with other non pharmacological treatment modalities and how
would you approach this patient as a treating physician?
Ans- The treatment
modalities given to this patient includes:
1.Meropenem:
MOA: Carbapenems are bactericidal beta-lactam
antibiotics that bind to penicillin-binding proteins (PBPs). By binding and
inactivating these proteins, carbapenems inhibit the synthesis of the bacterial
cell wall, which leads to cell death.
Indication: To prevent septic complications of acute
pancreatitis
Efficacy: Preventing septic complications of patients
with severe acute pancreatitis.
Reference link: https://pubmed.ncbi.nlm.nih.gov/14576501/#:~:text=Meropenem%20is%20as%20effective%20as,patients%20with%20severe%20acute%20pancreatitis.
2.Metronidazole:
MOA : Metronidazole diffuses into the
organism, inhibits protein synthesis by interacting with DNA and causing a loss
of helical DNA structure and strand breakage. Therefore, it causes cell death.
Indication: Preventing septal complications of acute
pancreatitis.
Efficacy: Metronidazole with Carbapenems is
successful in treatment of acute pancreatitis. Combination therapy with
Metronidazole reduces risk of drug resistance.
3.Amikacin:
MOA: It binds to bacterial 30S ribosomal
subunits and interferes with mRNA binding and t-RNA acceptor sites, interfering
with bacterial growth
Indication: prevent septal complications of acute
pancreatitis
Efficacy: Is being widely used in abdominal sepsis
because of appropriate efficacy against invasive gram negative bacteria.
B) Link to patient details:
https://nehae-logs.blogspot.com/2021/05/case-discussion-on-25-year-old-male.html
1) What is causing
the patient's dyspnea? How is it related to pancreatitis?
Ans- With severe
pancreatitis there are a lot of inflammatory chemicals that are secreted into
the blood stream. These chemicals create inflammation throughout the body,
including the lungs. As a result, a person may experience an inflammatory type
of reaction in the lungs called ARDS. Specifically, the small air sacs inside
the lungs called the alveoli can get inflamed and become filled with fluid
causing acute respiratory distress syndrome.
Acute pancreatitis can cause chemical changes in your
body that affect your lung function, causing the level of oxygen in your blood
to fall to dangerously low levels.
Reference link: https://www.mayoclinic.org/diseases-conditions/pancreatitis/symptoms-causes/syc-20360227
2) Name possible
reasons why the patient has developed a state of hyperglycemia.
Ans- It is possible
that the patient might have de novo diabetes secondary to pancreatitis. As
there is destruction of Beta cells in the islets of Langerhans some patients
are susceptible to hyperglycemia.
3) What is the
reason for his elevated LFTs? Is there a specific marker for Alcoholic Fatty
Liver disease?
Ans- As the patient has been
diagnosed with acute cholecystitis, that could be the possible reason for
elevated LFT markers. Elevated Lipase and amylase are also considered a
diagnostic of acute pancreatitis.
Alanine
Aminotransferase is a potential marker for alcoholic fatty liver disease but
much is needed in this field.
4) What is the line
of treatment in this patient?
Ans- Treatment plan of
this patient includes the following modalities:
·
Intravenous fluids
·
Pantoprazole
·
Ondansetron
·
Tramadol
·
Paracetamol
C) Link to patient details:
https://chennabhavana.blogspot.com/2021/05/general-medicine-case-discussion-1.html
Questions :-
1) What is the most
probable diagnosis in this patient?
Ans- The most probably
diagnosis is there is abdominal hemorrhage. This will give reasoning to the
abdominal distention, and the blood which is aspirated.
Differential
Diagnosis:
·
Ruptured Liver Abscess.
·
Organized collection secondary to Hollow viscous Perforation.
·
Organized Intraperitoneal Hematoma.
·
Free fluid with internal echoes in Bilateral in the Subdiaphragmatic
space.
·
Grade 3 RPD of right Kidney
2) What was the
cause of her death?
Ans- Cause of her death can be
due to complications of laparotomy surgery such as, hemorrhage (bleeding),
infection, or damage to internal organs.
Or, Septicemia causing multiorgan failure can also be
the probable cause of her death.
3) Does her NSAID
abuse have something to do with her condition? How?
Ans- NSAID abuse should be considered because-
· NSAID-induced
renal dysfunction has a wide spectrum of negative effects, including decreased
glomerular perfusion, decreased glomerular filtration rate, and acute renal
failure.
· Chronic
NSAIDs use has also been related to hepatotoxicity.
· While
the major adverse effects of NSAIDs such as gastrointestinal mucosa injury are
well known.
· NSAIDs
have also been associated with hepatic side effects ranging from asymptomatic
elevations in serum aminotransferase levels and hepatitis with jaundice to
fulminant liver failure and death.
5) Nephrology (and Urology) 10 Marks
A) Link to patient details:
https://kavyasamudrala.blogspot.com/2021/05/medicine-case-discussion-this-is-online.html
1. What could be
the reason for his SOB ?
Ans- His SOB was probably
due to Acidosis which was caused by Diuretics.
2. Why does he have
intermittent episodes of drowsiness ?
Ans- Hyponatremia appears
the most probable cause for his drowsiness.
3. Why did he
complaint of fleshy mass like passage in his urine?
Ans- Plenty of pus
cells in his urine passage appeared as
fleshy mass like
passage to him.
4. What are the
complications of TURP that he may have had?
Ans- The
possible risks of TURP include the following:
- · Bladder
injury.
- · Bleeding.
- · Blood
in the urine after surgery.
- · Electrolyte
abnormalities.
- · Infection.
- · Loss
of erections.
- · Painful
or difficult urination.
- · Retrograde
ejaculation
B) Link to patient details:
https://drsaranyaroshni.blogspot.com/2021/05/an-eight-year-old-with-frequent.html
Questions-
1.Why is the child excessively
hyperactive without much of social etiquettes ?
Ans- The exact pathophysiology of
Attention Deficit Hyperactivity Disorder (ADHD) is not clear. With this said,
several mechanisms have been proposed such as
·
Abnormalities
in the functioning of neurotransmitters, brain structure and cognitive
function.
·
Due to
the efficacy of medications such as psychostimulants and noradrenergic
tricyclics in the treatment of ADHD, neurotransmitters such as dopamine and
noradrenaline have been suggested as key players in the pathophysiology of
ADHD.
2. Why doesn't the child have the
excessive urge of urination at night time ?
Ans- The child may be
having psychosomatic urge to urinate during the day but this will not be
present during sleep as he will not be conscious.
3. How would you want to manage
the patient to relieve him of his symptoms?
Ans- The ideal management
would be-
· Urinating
on schedule and gradually spacing the time between bathroom visits.
· Medications
can include Botox injection as it helps bladder relax.
· Nerve
stimulation: This includes some of the latest treatment options for OAB. They
sometimes may help when there is no improvement with medications.
https://www.webmd.com/urinary-incontinence-oab/causes-overative-bladder
6) Infectious
Disease (HI virus, Mycobacteria, Gastroenterology, Pulmonology) 10
Marks
A) Link to patient details:
https://vyshnavikonakalla.blogspot.com/2021/05/a-40-year-old-lady-with-dysphagia-fever.html
Questions:-
1.Which clinical
history and physical findings are characteristic of tracheo esophageal fistula?
Ans- The Clinical history and physical
findings which are characteristic of tracheo esophageal fistula are-
·
Cough since 2 months on taking food and
liquids
·
Difficulty in swallowing since 2 month .
It was initially difficult only with solids but then followed by liquids also.
·
Laryngeal crepitus- positive
2) What are the
chances of this patient developing immune reconstitution inflammatory syndrome?
Can we prevent it?
Ans- Immune Reconstitution
Inflammatory Syndrome or IRIS is seen patients undergoing ART for RVD. In these
patients as there is immunosuppression because of ART, a previous opportunistic
infection can reactivate and give an exaggerated response.
Candida is an opportunistic pathogen hence it
is possible for this patient developing IRIS in response to a fresh candida
infection
The drug of choice in this infection would be
Fluconazole.
7) Infectious disease and
Hepatology:
A) Link to patient details:
https://kavyasamudrala.blogspot.com/2021/05/liver-abscess.html
1. Do you think drinking locally
made alcohol caused liver abscess in this patient due to predisposing factors
present in it ? What could
be the cause in this patient ?
Ans- The primary etiology of patient's condition
is probably Alcoholism. The consumption of locally brewed alcohol could be an
additional cause as there are high chances of improper filtration being done
which could be the cause of amoebic or pyogenic liver abscess. Poor economic
conditions lack of sanitation and malnutrition could also play a role as
predisposing factors.
2. What is the etiopathogenesis
of liver abscess in a chronic alcoholic patient ? ( since 30 years - 1
bottle per day)
Ans- Etiologic factors:
· Entry
of pathogen
· Content
of alcohol
· Cirrhotic
condition of liver
· Immune
status of the host
· Nutritional
status of the host
· Sanitary
conditions
Pathogenesis:
· Alcohol
induced hepatotoxicity
· Depression
of immune system due to alcoholism
· Poor
nutritional status

3. Is liver abscess more common
in right lobe ?
Ans- Right hepatic
lobe is larger than the left hepatic lobe. Therefore more blood supply to the
right lobe and hence more chances of pathogens entering the liver via the right
lobe through the hematogenous route.
4.What are the indications for
ultrasound guided aspiration of liver abscess ?
Ans- Indications for USG
guided aspiration of liver abscess
1. Large
abscess more than 6cms
2. Left
lobe abscess
3. Caudate
lobe abscess
4. Abscess
which is not responding to drugs
B) Link to patient details:
https://63konakanchihyndavi.blogspot.com/2021/05/case-discussion-on-liver-abcess.html
QUESTIONS:
1) Cause of liver abcess in this
patient ?
Ans-
Most common cause of a liver abscess is amoebic infection are caused by
Entamoeba histolytica.
The pyogenic abscesses can also be a potential cause
by bacteria that include E.coli, Klebsiella, Streptococcus, Staphylococcus, and
anaerobes.
2) How do you approach this
patient ?
Ans-
Treatment approach includes the following:
- · Sulbactam
+ Cefoperazone
- · Metronidazole
- · Optineurin
- · Tramadol
- · Acetaminophen
- · Paracetamol
3) Why do we treat here ; both
amoebic and pyogenic liver abcess?
Ans- We treat the paient for both amoebic and pyogenic abcess so that we dont rely only on anti-amebic therapy and insure comple treatment of the cause
4) Is there a way to confirmthe
definitive diagnosis in this patient?
Ans- Aspiration and culture of the aspirated fluid can help us draw a definitive diagnosis
8) Infectious disease (Mucormycosis, Ophthalmology, Otorhinolaryngology, Neurology) 10 Marks
A) Link to patient details:
http://manikaraovinay.blogspot.com/2021/05/50male-came-in-altered-sensorium.html
Questions :
1) What is the evolution of the symptomatology in this patient in terms of
an event timeline and where is the anatomical localization for the problem and
what is the primary etiology of the patient's problem?
Ans-
The evolution if symptomatology is as follows:
- · Diagnosed
with hypertension 3 years ago
- · Fever
since 10 days
- · Facial
puffiness, periorbital edema and Right sided hemiparesis since 4 days
· Altered
sensorium since 2 days
Anatomical localization: Infarcts in frontal and
temporal lobes of brain
Primary etiology: Mucormycetes infection causing
rhino-orbito-cerebral mucormycosis
2) What is the
efficacy of drugs used along with other non pharmacological treatment
modalities and how would you approach this patient as a treating
physician?
Ans- The treatment modality in this patient includes:
1.Itraconazole:
MOA: Itraconazole acts by inhibiting the fungal
cytochrome P-450 dependent enzyme lanosterol 14-α-demethylase. When this enzyme
is inhibited it blocks the conversion of lanosterol to ergosterol, which
disrupts fungal cell membrane synthesis
Indication: Itraconazole is the only marketed
azole drug that has in vitro activity against Mucorales. There are case reports
of successful therapy with itraconazole alone .However, as mentioned above,
itraconazole prophylaxis has been described as a risk factor for breakthrough
mucormycosis
3) What are the
postulated reasons for a sudden apparent rise in the incidence of mucormycosis
in India at this point of time?
Ans- The reasons for sudden rise of mucormycosis cases
in India include:
- · COVID-19
infection among diabetic patients in whom there is lower immunity.
- · Increased
dose of steroid usage and also because of lower availability of remdesivir ,
tocilizumab leading to dependence on steroids for treatment.
- · Use
of ordinary water instead of sterile water in humidifiers.
- · Prolonged
ICU stay
Comments
Post a Comment